
Around the world, nursing is consistently identified as the backbone of health care delivery. Nurses are the largest segment of the healthcare workforce, the primary coordinators of care, and, for millions of people, the only accessible health professional in their community. This essential role is supported by a robust foundation of nursing education and research, which prepares nurses to address complex health needs, advance evidence-based practice, and respond to evolving public health challenges.
Any policy that undermines these postgraduate or graduate educational pathways threatens not only the profession locally, but the quality and safety of care across health systems. Therefore, when the United States Department of Education proposes a federal definition that excludes nursing graduate study from the category of a “professional degree,” the implications stretch far beyond U.S. borders.
This is not simply an American policy debate; it is a warning sign for the global health community.
At a time when health systems are already strained, classifying nursing threatens the pipeline of advanced practice nurses, widens inequities, and undermines the scientific foundation of the discipline itself.
The Global Stakes: Why International Nurses Should Care
Even though the proposed policy is U.S.-specific, similar patterns can spread worldwide:
- When one country downgrades or undermines nursing education, others may follow.
- International regulatory bodies often align their standards with larger or more outspoken systems.
- Global perceptions of nursing are shaped by cultural signals from well-resourced health systems, such as in the U.S.
Classifying graduate nursing as something other than a professional degree reinforces outdated beliefs that nursing is subordinate, task-oriented, or lacking scientific grounding. These misconceptions continue to limit nursing autonomy, leadership, and scope of practice in many regions.
Decisions like this, regardless of where they originate, risk strengthening harmful biases about the profession and can undermine global efforts to elevate nursing as a knowledge-driven, evidence-based discipline.
What Is Being Proposed in the U.S., in Brief
Under the One Big Beautiful Bill Act (OBBBA), the U.S. Department of Education must determine which graduate programs qualify for higher federal loan limits. Degrees such as medicine, law, and theology are included. Nursing is not.
If this exclusion moves forward, students pursuing graduate nursing degrees (MSN, PhD, APRN, CRNA, CNM, CNS) could face restricted financial aid, making advanced nursing education harder to access.
While some argue the change may affect only a minority of students, the broader consequences for the nursing workforce and profession, and ultimately for patient care, may be significant.
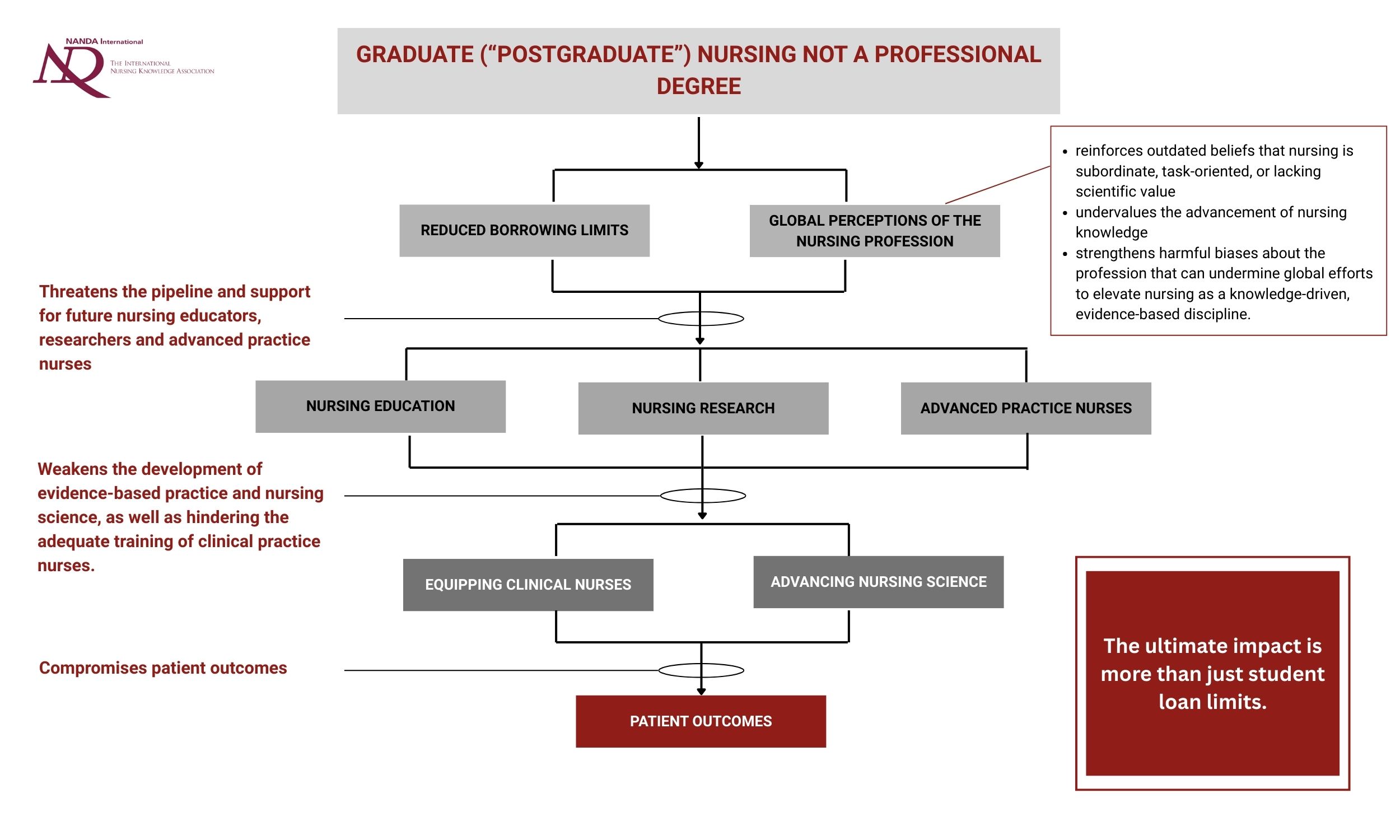
Summary of the flow-on effects through the nursing profession and ultimately to patient outcomes.
Impact on Nursing Research and Education
Policies that alter how nursing is classified, whether in the U.S., Europe, Asia, Africa, Latin America, or Oceania, tend to reflect broader societal attitudes about the profession. These attitudes shape how nursing is funded, supported, and understood as a scientific discipline. When any nation questions or constrains nursing’s status as a professional field, downstream effects emerge that resonate across the global nursing community.
A central concern is how such decisions weaken the foundation of nursing research and nursing education, the mechanisms that drive innovation, improve patient outcomes, and ensure high-quality workforce preparation.
A decision like this
Signal that nursing knowledge is undervalued
- Classifying nursing as less than a professional field sends a message that the discipline’s scientific foundation is not fully recognized, which can weaken the perceived legitimacy of nursing scholarship.
Threatens the pipeline of future educators and researchers
- Graduate and doctoral programs prepare faculty, researchers, clinical scholars, and advanced practice clinicians. Restricting access to these programs shrinks the pool of future nurse educators and researchers, worsening existing shortages worldwide.
- Professional‐degree status may influence visa eligibility, institutional funding mechanisms, and program recognition. If nursing’s status is weakened, international nurses, who already face financial and administrative barriers, may find U.S. graduate programmes less accessible. This creates a risk of also narrowing the global pipeline of future nurse educators and researchers.
May reduce investment in nursing research
- When graduate study is viewed as less “professional,” universities and funders tend to be less likely to prioritize nursing research. This may limit research capacity, slow innovation, and constrain the discipline’s ability to generate evidence to improve patient care.
Weakens the development of evidence-based practice
- Reduced scholarly output erodes nursing’s scientific visibility and restricts the growth of evidence needed to support safe, high-quality care across health systems.
In short, weakening the status of graduate nursing education creates long-term barriers to building faculty capacity, advancing nursing science, supporting mobility for international students, and sustaining a resilient, well-prepared global nursing workforce.
Impact on Clinical Practice and Patient Outcomes
Graduate education is essential, not optional, for healthcare systems
Graduate nursing education is not a luxury; it is the backbone of safe, high-quality clinical care. Advanced practice nurses, including Clinical Nurse Specialists (CNSs), Nurse Practitioners, CRNAs, CNMs, and nurses prepared at the doctoral level (educators, researchers, administrators, practice experts) are central to improving patient outcomes, strengthening health system performance, and advancing evidence-based practice across settings (Pate, Rutledge & Belin, 2024; Kerr, Donovan & McSorley, 2021; Klein, 2021; Tracy et al., 2020). Policies that restrict access to these graduate pathways directly diminish the clinical capacity of the healthcare workforce.
- Graduate education directly strengthens patient care and system performance
Advanced practice nurses provide expert assessment, diagnostic reasoning, consultation, and system-level leadership. CNSs, for example, are master’s- or doctoral-prepared clinicians whose work reduces complications, lengths of stay, and overall costs while increasing patient satisfaction. Their expertise supports nurses at the bedside, drives quality improvement, and promotes consistent use of evidence-based interventions.
The workforce pipeline that produces these clinicians is already under strain. A recent analysis shows that senior nursing faculty are retiring faster than new doctoral-prepared educators can replace them, creating a widening gap in the capacity to educate the next generation (Fang, Donovan, & McSorley, 2021). This shortage has direct clinical consequences: insufficient faculty limits enrollment, slows the development of clinical reasoning curricula, and ultimately affects how well prepared new nurses are to manage complex patient needs.
As Campbell, Miehe, and Tice (2024) emphasize, inadequate development of clinical judgment among novice nurses contributes to errors and poorer outcomes. When access to graduate education is restricted, the system loses both advanced clinicians and the faculty who teach foundational skills. Fewer pathways to advanced training therefore translate into fewer clinicians equipped to deliver the level of care modern health systems require.
- Equity and diversity in advanced practice, and patient outcomes, will suffer
Financial barriers already disproportionately affect first-generation students, students of color, and those from low-income backgrounds. If nursing graduate programs become harder to access, the profession will lose critical diversity at the advanced practice level.
This loss is not merely symbolic. Decades of evidence show that a diverse healthcare workforce improves communication, trust, satisfaction, and outcomes, particularly in marginalized communities (Institute of Medicine [IOM], 2004; Saha et al., 2008; Marrast et al., 2014; Gomez & Bernet, 2019). Reducing access to graduate education risks narrowing the pipeline of diverse advanced practice leaders, thereby widening existing disparities in both care access and patient experience.
- Limiting advanced training undermines clinical safety and quality
Graduate education equips nurses with the analytical, diagnostic, and leadership skills essential for managing today’s patient populations. Without adequate preparation, fewer clinicians can:
-
- manage complex chronic diseases
- perform advanced assessment and diagnostic reasoning
- deliver trauma-informed and culturally responsive care
- lead quality improvement and safety initiatives
- coordinate care across fragmented systems
When fewer nurses hold advanced practice credentials, health systems experience increased fragmentation of care, longer wait times, and reduced capacity to manage high-acuity or chronically complex patients. The result is predictable: diminished safety, greater variability in care quality, and more strain on already overburdened teams.
Where NANDA®-I Fits Into This Moment
Nursing is not defined by tasks. It is a discipline built on theory, empirical science, clinical reasoning, and a unique body of knowledge.
NANDA-I’s work in developing standardized nursing language strengthens this scientific foundation. It makes nursing knowledge visible, measurable, and actionable, clearly demonstrating that nurses identify, assess, and treat human responses to health and illness in ways no other discipline does.
At a moment when policy threatens to diminish nursing’s educational standing, NANDA-I’s mission is more critical than ever:
- to demonstrate nursing’s distinct disciplinary voice,
- to show that nursing knowledge is scientific, evidence-based, and indispensable, and
- to ensure that nurses’ contributions are recognized and valued across health systems.
This classification of the nursing profession does not only threaten funding here in the U.S.; it threatens the recognition of nursing as a scholarly, autonomous profession.
What Nurses Can Do Now
Public comments are open, and collective advocacy matters. The nursing profession must respond: loudly, clearly, and globally.
✍️ Add your name to the ANA petition urging the Department of Education to include nursing within the definition of “professional degree”: https://ana.quorum.us/campaign/professionaldegreepetition/
Whether you are a nurse in the United States, Canada, India, Brazil, Australia, the UK, South Africa, or anywhere in the world, your voice reinforces a universal truth: nursing is a profession defined by knowledge, expertise, and irreplaceable impact on patient health.
If the U.S. weakens its support for nursing education, the consequences will likely reverberate across global healthcare systems.
Now is the moment to stand up: for nursing, for patients, and for the future of our profession.
References
Campbell, J., Miehe, J., & Tice, M. (2024). Faculty development on the use of a clinical judgment model in the pre-licensure nursing curriculum. Journal of Professional Nursing, 51, 9–15. https://doi.org/10.1016/j.profnurs.2023.11.003
Fang, D., Donovan, M., & McSorley, O. (2021). Assessment of nursing faculty retirement projections. Nursing Outlook, 72(2), 102135. https://doi.org/10.1016/j.outlook.2020.11.007
Gomez, L. E., & Bernet, P. (2019). Diversity improves performance and outcomes. Health Affairs, 38(2), 310–316. https://doi.org/10.1377/hlthaff.2018.0829
Institute of Medicine. (2004). In the nation’s compelling interest: Ensuring diversity in the health-care workforce. National Academies Press. https://pubmed.ncbi.nlm.nih.gov/25009857/
Kerr, H., Donovan, M., & McSorley, O. (2021). Evaluation of the role of the clinical nurse specialist in cancer care: An integrative literature review. European Journal of Cancer Care, 30(3), e13415. https://doi.org/10.1111/ecc.13415
Klein, E. (2021). Clinical nurse specialists: Leaders in improving patient outcomes. Clinical Nurse Specialist, 35(6), 281–283. https://doi.org/10.1097/NUR.0000000000000644
Marrast, L. M., Zallman, L., Woolhandler, S., Bor, D. H., & McCormick, D. (2014). Minority physicians’ role in caring for underserved patients: Implications for workforce diversity. International Journal of Health Services, 44(3), 506–524. https://doi.org/10.2190/HS.44.3.g
Pate, K. D., Rutledge, S. R., & Belin, L. D. (2024). Clinical nurse specialists using evidence-based practice to prevent falls. Clinical Nurse Specialist, 38(1), 18–24. https://doi.org/10.1097/NUR.0000000000000791
Saha, S., Beach, M. C., & Cooper, L. A. (2008). Patient centeredness, cultural competence and healthcare quality. Journal of the National Medical Association, 100(11), 1275–1285. https://pmc.ncbi.nlm.nih.gov/articles/PMC2824588/
Tracy, M. F., Oerther, S., Arslanian-Engoren, C., Girouard, S., Minarik, P., Patrician, P., Vollman, K., Sanders, N., McCausland, M., Antai-Otong, D., & Talsma, A. (2020). Improving the care and health of populations through optimal use of clinical nurse specialists. Nursing Outlook, 68(4), 523–527. https://doi.org/10.1016/j.outlook.2020.06.004
Comments (0)
Leave a comment