Nursing Assessments (From Assessment to Diagnosis)
Definition and Importance
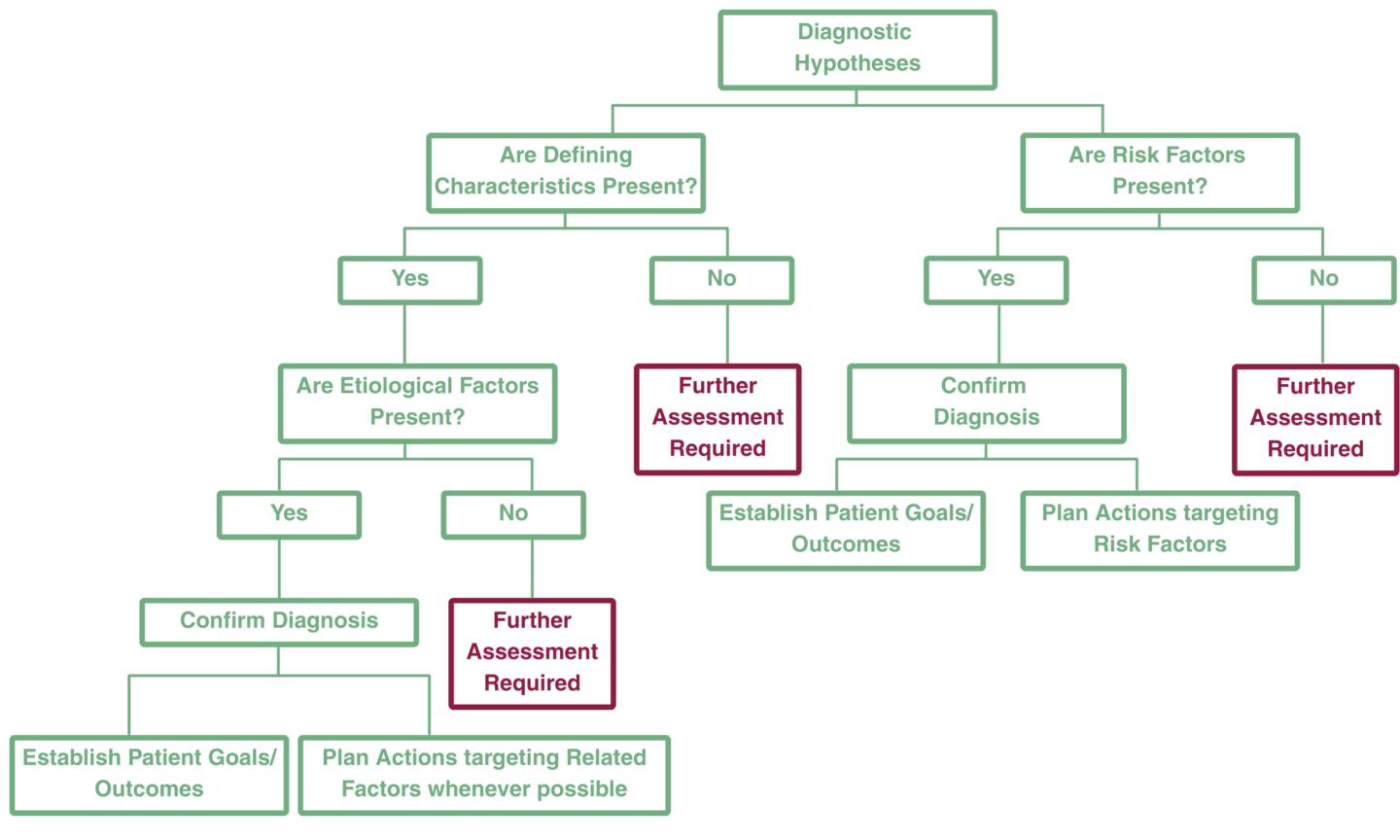
Assessment is the foundation of nursing practice. It supplies the raw observations, measurements, and patient reports nurses need to make clinical judgments about human responses to health conditions and life processes. Moving from assessment to diagnosis is an iterative process: nurses collect data, interpret and cluster findings into meaningful patterns, generate diagnostic hypotheses, validate or refute them, and then prioritize and document diagnoses that guide care.
This process can proceed in a stepwise fashion in some cases, but often requires a back-and-forth movement between steps as more data are identified, leading to additional questions or the need to obtain different data. Hypotheses are challenged, refuted, and sometimes the process must begin again. The nurse’s ability to build rapport with the patient, family, or group is critical to obtaining a comprehensive assessment.
INKA (formerly NANDA® International, NANDA-I) emphasizes assessment because accurate nursing diagnoses depend on accurate, meaningful, and complete nursing data.

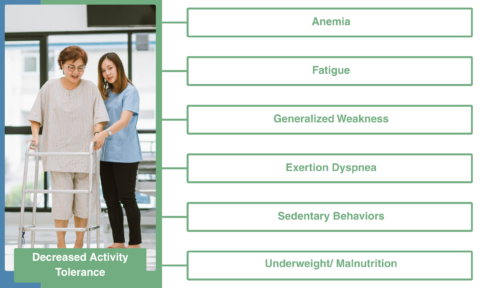 Collected data are raw until nurses apply conceptual knowledge to interpret them. Data analysis transforms measurements and observations into meaningful information (for example, converting height/weight to BMI and interpreting a BMI of 18.4 as underweight).
Collected data are raw until nurses apply conceptual knowledge to interpret them. Data analysis transforms measurements and observations into meaningful information (for example, converting height/weight to BMI and interpreting a BMI of 18.4 as underweight).